


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Prevenar 13 contains the 7 pneumococcal capsular polysaccharides that are in pneumococcal 7-valent conjugate vaccine (4, 6B, 9V, 14, 18C, 19F, 23F) plus 6 additional polysaccharides (1, 3, 5, 6A, 7F, 19A) all conjugated to CRM197 carrier protein.
Children 6 weeks to 5 years of age: Based on serotype surveillance in Europe performed before the introduction of pneumococcal 7-valent conjugate vaccine, Prevenar 13 is estimated to cover 73%-100% (depending on the country) of serotypes causing invasive pneumococcal disease (IPD) in children less than 5 years of age. In this age group, serotypes 1, 3, 5, 6A, 7F, and 19A account for 15.6% to 59.7% of invasive disease, depending on the country, the time period studied, and the use of pneumococcal 7-valent conjugate vaccine.
Acute otitis media (AOM) is a common childhood disease with different aetiologies. Bacteria can be responsible for 60%-70% of clinical episodes of AOM. Streptococcus pneumoniae is one of the most common causes of bacterial AOM worldwide.
Prevenar 13 is estimated to cover over 90% of serotypes causing antibiotic-resistant IPD.
Prevenar 13 Immunogenicity Clinical Studies: The protective efficacy of Prevenar 13 against IPD has not been studied. As recommended by the World Health Organization (WHO) the assessment of potential efficacy against IPD has been based on a comparison of immune responses to the seven common serotypes shared between Prevenar 13 and pneumococcal 7-valent conjugate vaccine, for which protective efficacy has been proven. Immune responses to the additional 6 serotypes were also measured.
Immune Responses Following a 3-Dose Primary Infant Series: Clinical studies have been conducted in a number of European countries and the US using a range of vaccination schedules, including two randomized non-inferiority studies (Germany using a 2, 3, 4 month primary series [006] and US using a 2, 4, 6 month primary series [004]). In these two studies pneumococcal immune responses were compared using a set of non-inferiority criteria including the percentage of subjects with serum anti-polysaccharide serotype specific IgG ≥0.35 µg/mL one month after the primary series and the comparison of IgG geometric mean concentrations (ELISA GMCs); in addition, functional antibody titres (OPA) between subjects receiving Prevenar 13 and pneumococcal 7-valent conjugate vaccine were compared. For the six additional serotypes, these values were compared with the lowest response among all of the seven common serotypes in the pneumococcal 7-valent conjugate vaccine recipients.
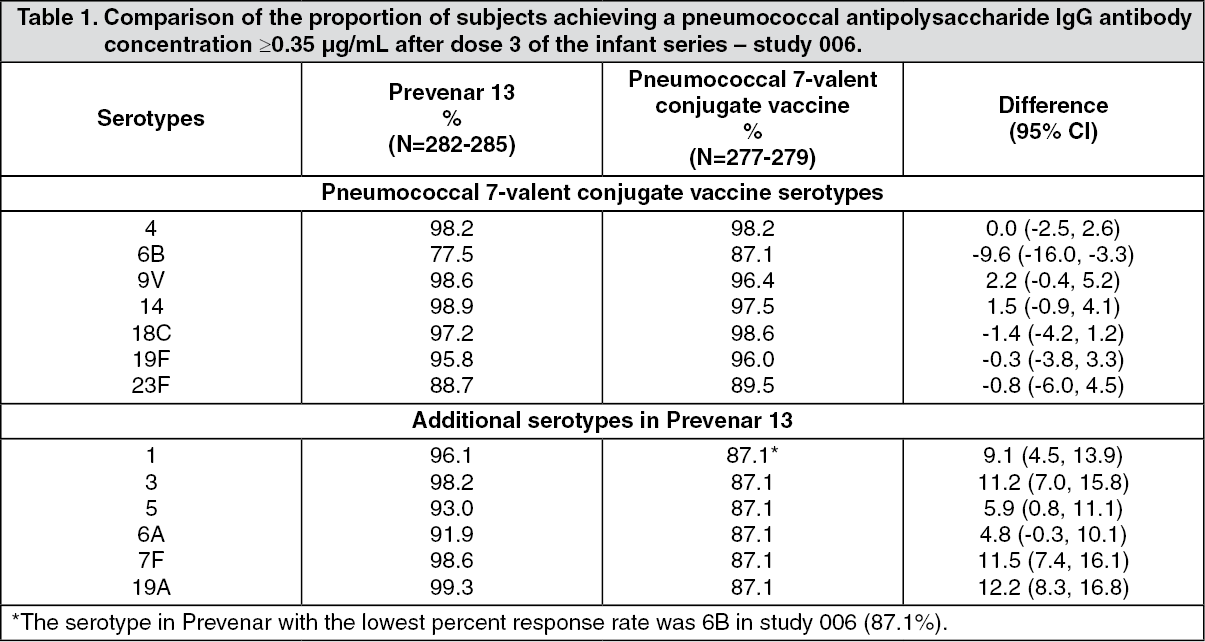
The non-inferiority immune response comparisons for study 006, based on the proportion of infants achieving anti-polysaccharide IgG concentrations ≥0.35 µg/mL, are shown in Table 1. Results for study 004 were similar. Prevenar 13 non-inferiority (lower bound of the 95% CI for the difference in percentage of responders at 0.35 µg/mL between groups was >-10%) was demonstrated for all 7 common serotypes, except for serotype 6B in study 006 and serotypes 6B and 9V in study 004, which missed by a small margin. All seven common serotypes met pre-defined non-inferiority criteria for IgG ELISA GMCs. Prevenar 13 elicited comparable, although slightly lower, antibody levels than pneumococcal 7-valent conjugate vaccine for the 7 common serotypes. The clinical relevance of these differences is not known.
Non-inferiority was met for the 6 additional serotypes based on the proportion of infants achieving antibody concentrations ≥0.35 µg/mL and comparison of IgG ELISA GMCs in study 006 and was met for 5 out of the 6 serotypes, with the exception of serotype 3 for study 004. For serotype 3, the percentage of Prevenar 13 recipients with serum IgG ≥0.35 µg/mL were 98.2% (study 006) and 63.5% (study 004). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevenar 13 elicited functional antibodies to all 13 vaccine serotypes in studies 004 and 006. For the 7 common serotypes there were no differences between groups in the proportion of subjects with OPA titres ≥1:8. For each of the seven common serotypes, >96% and >90% of the Prevenar 13 recipients reached an OPA titre ≥1:8 one month after the primary series in studies 006 and 004, respectively.
For each of the 6 additional serotypes, Prevenar 13 elicited OPA titres ≥1:8 in 91.4% to 100% of vaccinees one month after the primary series in studies 004/006. The functional antibody (OPA) geometric mean titres for serotypes 1, 3 and 5 were lower than the titres for each of the other additional serotypes; the clinical relevance of this observation for protective efficacy is unknown.
Immune Responses Following a 2-Dose Primary Series: The immunogenicity after 2 doses in infants has been documented in four studies. The proportion of infants achieving a pneumococcal anti-capsular polysaccharide IgG concentration ≥0.35 μg/mL one month after the second dose ranged from 79.6% to 98.5% across 11 of the 13 vaccine serotypes. Smaller proportions of infants achieved this antibody concentration threshold for serotype 6B (27.9% to 57.3%) and 23F (55.8% to 68.1%) for all studies using a 2, 4 month regimen, compared to 58.4% for serotype 6B and 68.6% for 23F for a study using a 3, 5 month regimen. After the booster dose, all vaccine serotypes including 6B and 23F had immune responses consistent with adequate priming with a 2-dose primary series. In a UK study, the functional antibody (OPA) responses were comparable for all serotypes including 6B and 23F in the pneumococcal 7-valent conjugate vaccine and Prevenar 13 arms after the primary series at 2 and 4 months of age and after the booster dose at 12 months of age. For Prevenar 13 recipients, the proportion of responders with an OPA titre ≥1:8 was at least 87% following the infant series, and at least 93% following the booster dose. The OPA geometric mean titres for serotypes 1, 3 and 5 were lower than the titres for each of the other additional serotypes; the clinical relevance of this observation is unknown.
Booster Responses Following 2-Dose and 3-Dose Primary Series: Following the booster dose, antibody concentrations increased from the pre-booster level for all 13 serotypes. Post-booster antibody concentrations were higher for 12 serotypes than those achieved after the infant primary series. These observations are consistent with adequate priming (the induction of immunologic memory). The immune response for serotype 3 following the booster dose was not increased above the levels seen after the infant vaccination series; the clinical relevance of this observation regarding the induction of serotype 3 immune memory is unknown.
Antibody responses to booster doses following 2-dose or 3-dose infant primary series were comparable for all 13 vaccine serotypes.
For children aged from 7 months to 5 years, age appropriate catch-up immunization schedules (as described in Dosage & Administration) result in levels of anti-capsular polysaccharide IgG antibody responses to each of the 13 serotypes that are at least comparable to those of a 3-dose primary series in infants.
Long-term persistence of antibodies has not been investigated after administration of Prevenar 13 as either a primary series in infants plus booster or after administration of a single priming dose in older children. Since the introduction of pneumococcal 7-valent conjugate vaccine in 2000, pneumococcal disease surveillance data have not shown that the immunity elicited by pneumococcal 7-valent conjugate vaccine in infancy have waned over time.
Preterm Infants: Safety and immunogenicity of Prevenar 13 given at 2, 3, 4 and 12 months was assessed in 100 prematurely born infants (Estimated Gestational Age [EGA] mean, 31 weeks; range, 26 to 36 weeks) and compared with 100 infants born at term (EGA mean, 39 weeks; range, 37 to 42 weeks). More than 85% of subjects in the preterm group in the evaluable immunogenicity population achieved a pneumococcal polysaccharide IgG binding antibody concentration ≥0.35 µg/mL 1 month after the infant series for all serotypes except serotypes 5 (71.7%), 6A (82.7%), and 6B (72.7%) in the preterm group. For these 3 serotypes, the proportion of responders among preterm infants was significantly lower than among term infants. One month after the toddler dose, evidence of priming was observed as the proportion of subjects in each group in the evaluable toddler immunogenicity population achieving this same antibody concentration threshold was >97%, except for serotype 3 (70.6% in preterm infants and 79.3% in term infants). In general, serotype-specific IgG GMCs were lower for preterm infants than term infants.
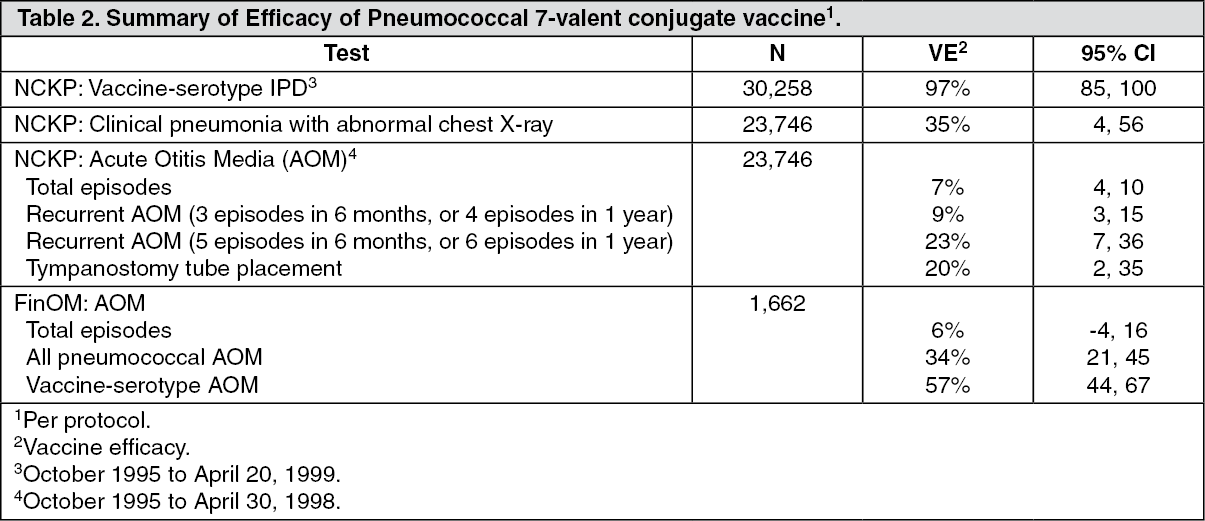
Pneumococcal 7-valent conjugate vaccine Protective Efficacy: The efficacy of pneumococcal 7-valent conjugate vaccine was evaluated in two major studies - the Northern California Kaiser Permanente (NCKP) study and the Finnish Otitis Media (FinOM) study. Both studies were randomised, double-blind, active-control studies in which infants were randomised to receive either pneumococcal 7-valent conjugate vaccine or control vaccine (NCKP, meningococcal serogroup C CRM-conjugate [MnCC] vaccine; FinOM, hepatitis B vaccine) in a 4-dose series at 2, 4, 6, and 12 - 15 months of age. The efficacy results from these studies (for invasive pneumococcal disease, pneumonia, and acute otitis media) are presented as follows (Table 2). (See Table 2.)
 Click on icon to see table/diagram/image
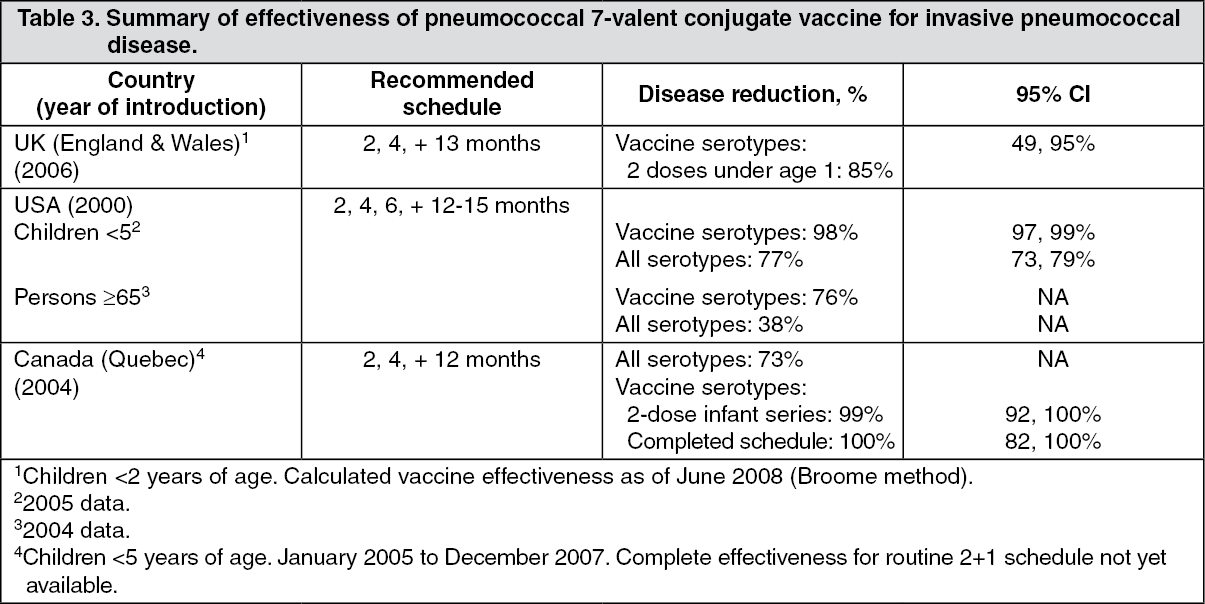
Click on icon to see table/diagram/imagePneumococcal 7-valent conjugate vaccine Effectiveness: The effectiveness (both direct and indirect effect) of pneumococcal 7-valent conjugate vaccine against pneumococcal disease has been evaluated in both 3-dose and 2-dose primary infant series immunization programs, each with booster doses (Table 3). Following the widespread use of pneumococcal 7-valent conjugate vaccine, the incidence of IPD has been consistently and substantially reduced. An increase in the incidence of IPD cases caused by serotypes not contained in pneumococcal 7-valent conjugate vaccine, such as 1, 7F and 19A, has been reported in some countries. Surveillance will continue with Prevenar 13, and as countries update their surveillance data, information in this table may change.
Using the screening method, serotype specific effectiveness estimates for 2 doses under the age of 1 year in the UK were 66% (-29, 91%) and 100% (25, 100%) for serotype 6B and 23F, respectively. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEffectiveness of pneumococcal 7-valent conjugate vaccine in a 3+1 schedule has also been observed against acute otitis media and pneumonia since its introduction in a national immunization program. In a retrospective evaluation of a large US insurance database, AOM visits were reduced by 42.7% (95% CI, 42.4%-43.1%), and prescriptions for AOM by 41.9%, in children younger than 2 years of age, compared with a pre-licensure baseline (2004 vs. 1997 -99). In a similar analysis, hospitalisations and ambulatory visits for all-cause pneumonia were reduced by 52.4% and 41.1%, respectively. For those events specifically identified as pneumococcal pneumonia, the observed reductions in hospitalisations and ambulatory visits were 57.6% and 46.9%, respectively, in children younger than 2 years of age, compared with a pre-licensure baseline (2004 vs. 1997 - 99). While direct cause-and-effect cannot be inferred from observational analyses of this type, these findings suggest that pneumococcal 7-valent conjugate vaccine plays an important role in reducing the burden of mucosal disease (AOM and pneumonia) in the target population.
Additional Pneumococcal 7-valent conjugate vaccine Immunogenicity Data: Children with Sickle Cell Disease: The immunogenicity of pneumococcal 7-valent conjugate vaccine has been investigated in an open-label, multicenter study in 49 infants with sickle cell disease. Children were vaccinated with pneumococcal 7-valent conjugate vaccine (3 doses one month apart from the age of 2 months), and 46 of these children also received a 23-valent pneumococcal polysaccharide vaccine at the age of 15 - 18 months. After primary immunization, 95.6% of the subjects had antibody levels of at least 0.35 µg/mL for all 7 serotypes found in pneumococcal 7-valent conjugate vaccine. A significant increase was seen in the concentrations of antibodies against the 7 serotypes after the polysaccharide vaccination, suggesting that immunological memory was well established.
Children and Adolescents 5-17 Years of Age: In Study 6096A1-3011 in the US, in children 5 to <10 years of age previously vaccinated with at least 1 dose of pneumococcal 7-valent conjugate vaccine, and in pneumococcal vaccine-naïve children and adolescents 10-17 years of age 1 dose of Prevenar 13 elicited immune responses to all 13 serotypes.
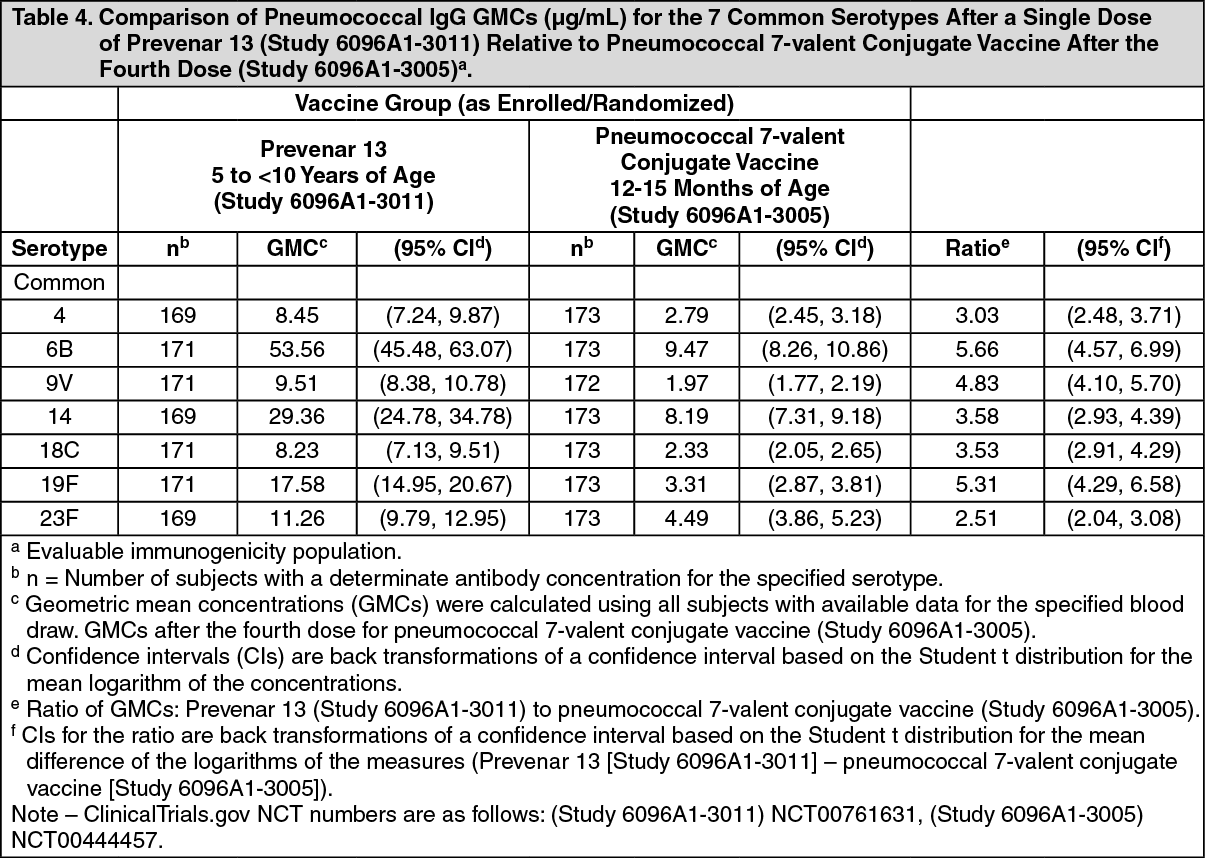
In children 5 to <10 years of age, serum IgG concentrations for the 7 common serotypes 1 month after administration of a single dose of Prevenar 13 vaccination (Study 6096A1-3011) were non-inferior (i.e., the lower limit of the 2-sided 95% CI for the geometric mean ratio [GMR] of >0.5) to those elicited by the fourth dose of pneumococcal 7-valent conjugate at 12-15 months of age (Study 6096A1-3005). In addition, IgG concentrations elicited by a single dose of Prevenar 13 for the 6 additional serotypes in children 5 to <10 years of age were non-inferior to those elicited by the fourth dose of Prevenar 13 at 12-15 months of age (Study 6096A1-3005) as shown in Tables 4 and 5. (See Tables 4 and 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image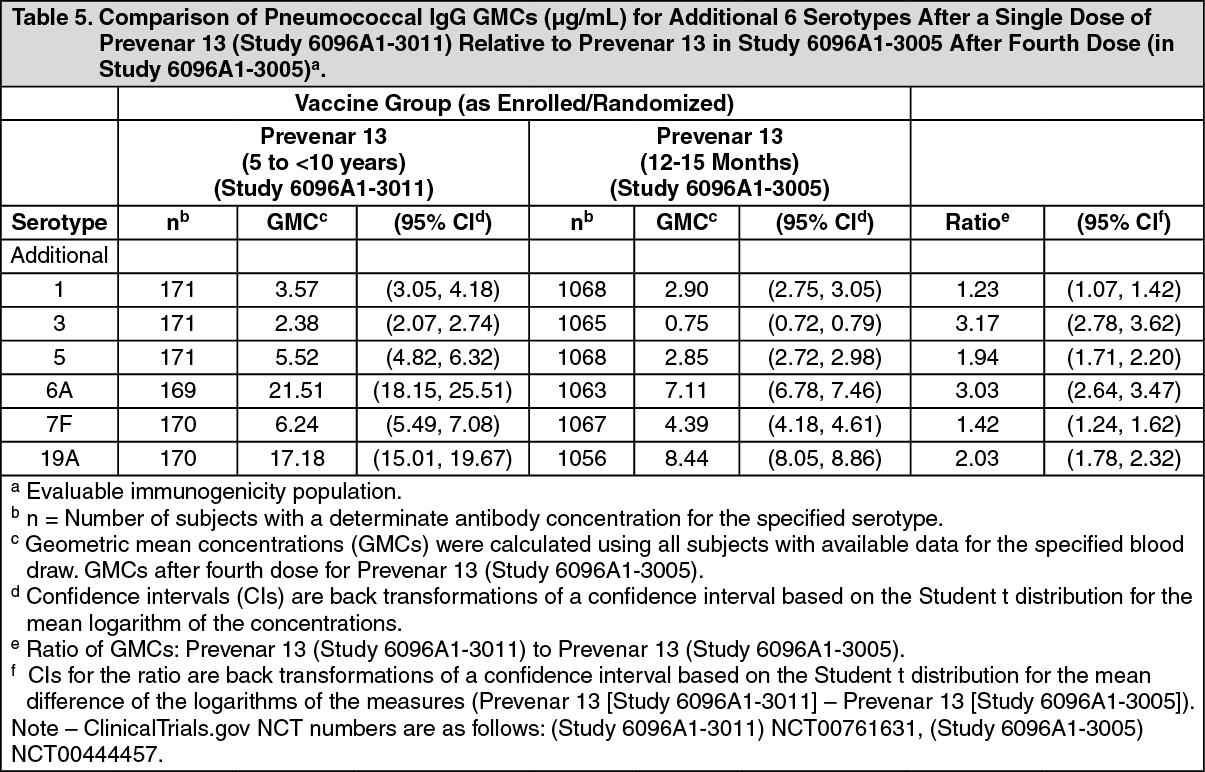 Click on icon to see table/diagram/image
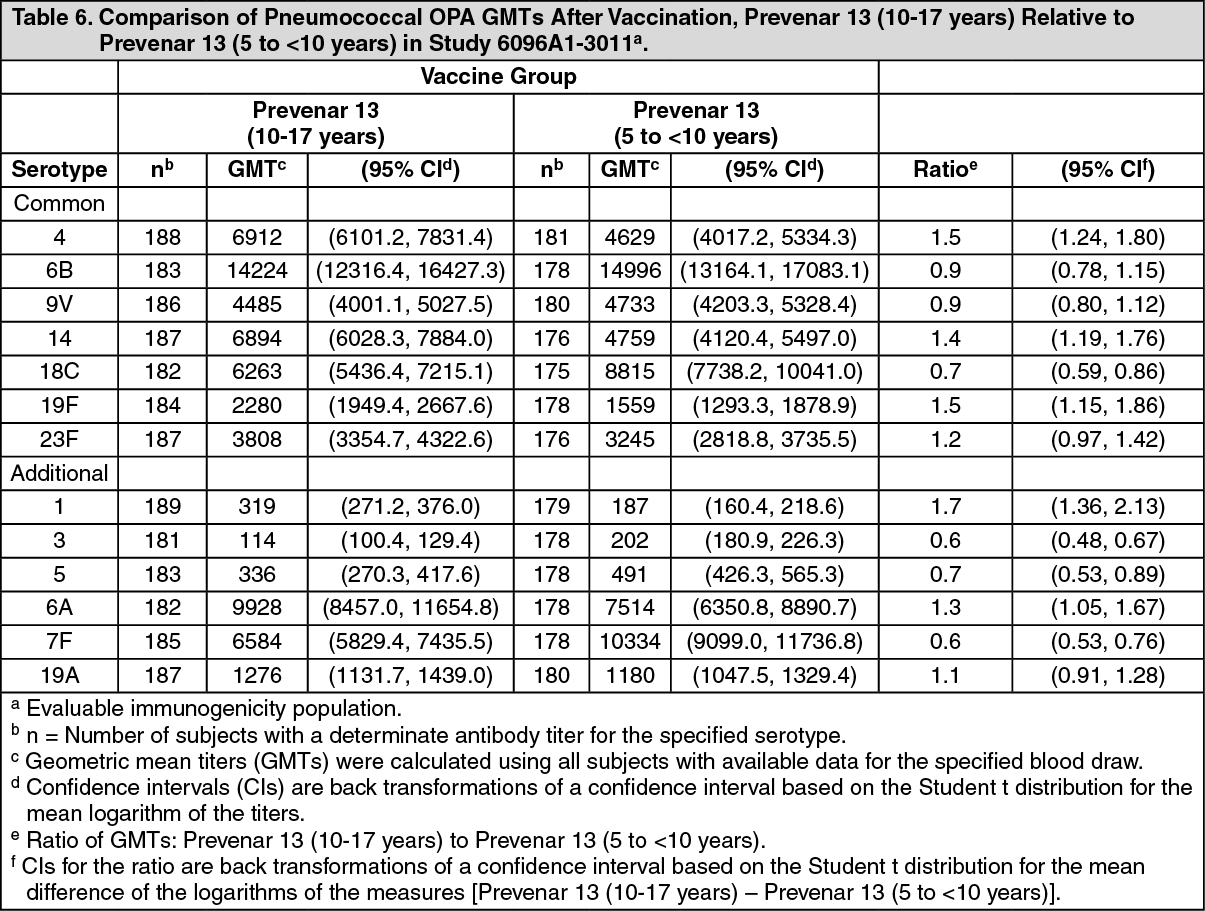
Click on icon to see table/diagram/imageIn children and adolescents 10-17 years of age opsonophagocytic activity (OPA) GMTs1 month after vaccination were non-inferior (i.e., the lower limit of the 2-sided 95% CI for the GMR of >0.5) to OPA GMTs in the 5 to <10 year old group for 12 of the 13 serotypes (except for serotype 3), as shown in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
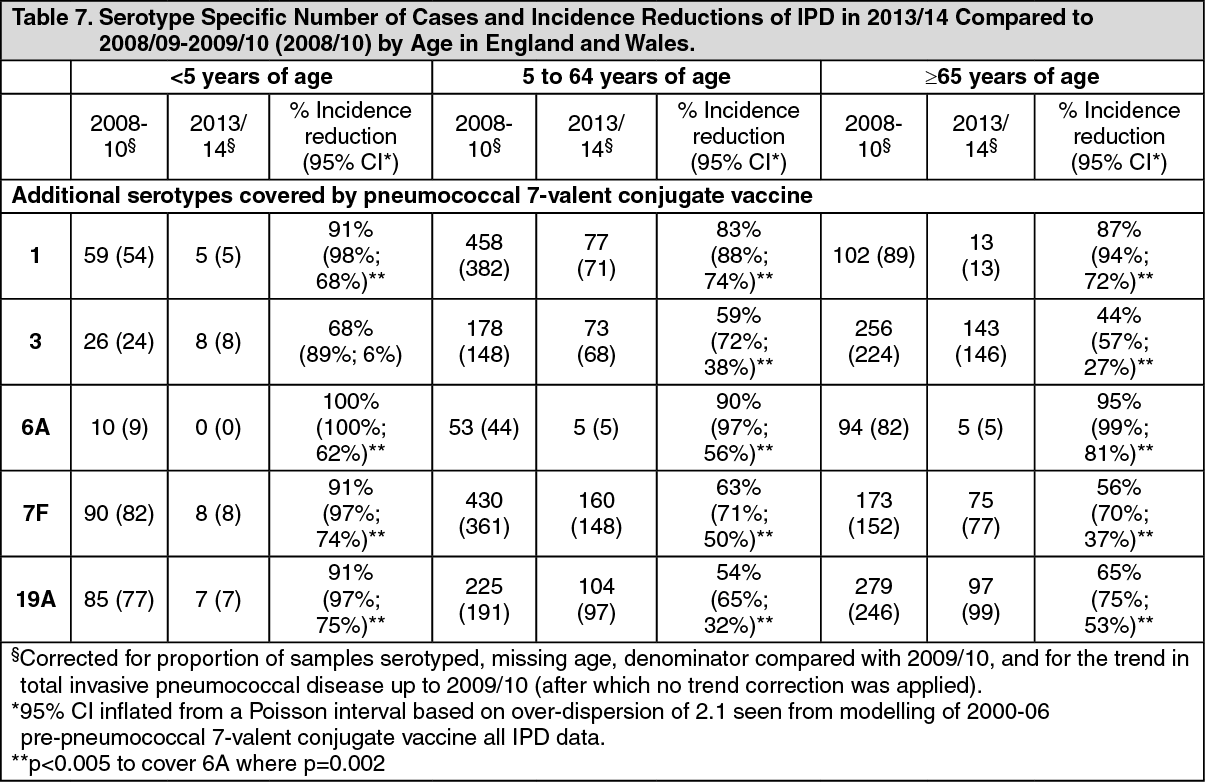
Click on icon to see table/diagram/imagePrevenar 13 Effectiveness: Invasive Pneumococcal Disease: Four years after the introduction of pneumococcal 7-valent conjugate vaccine as a two dose primary series plus booster dose in the second year of life and with a 94% vaccine uptake a 98% (95% CI 95; 99) reduction of disease caused by the 7 vaccine serotypes was reported in England and Wales. Subsequently, four years following the switch to Prevenar 13, the additional reduction in incidence of IPD due to the 7 serotypes in pneumococcal 7-valent conjugate vaccine ranged from 76% in children less than 2 years of age to 91% in children 5-14 years of age. The serotype specific reductions for each of the 5 additional serotypes in Prevenar 13 (no cases of serotype 5 IPD were observed) by age group are shown in Table 4 and ranged from 68% (serotype 3) to 100% (serotype 6A) for children less than 5 years of age. Significant incidence reductions were also observed in older age groups who had not been vaccinated with Prevenar 13 (indirect effect). (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOtitis Media (OM): In a two dose primary series plus booster dose in the second year of life the impact of Prevenar 13 on OM was documented in a population based active surveillance system in Israel with tympanocentesis culturing of middle ear fluid in children less than 2 years of age with OM. Following the introduction of pneumococcal 7-valent conjugate vaccine and subsequently Prevenar 13 there was a decline in incidence of 96% of OM for the pneumococcal 7-valent conjugate vaccine serotypes plus serotype 6A and a decline in incidence of 85% for the additional serotypes 1, 3, 5, 7F, and 19A in Prevenar 13.
In a prospective, population-based, long-term surveillance study conducted in Israel between 2004 and 2015 following the introduction of pneumococcal 7-valent conjugate vaccine and subsequently Prevenar 13, reductions of non-pneumococcal bacteria isolated from children <3 years of age with OM were 75% for all NTHi cases, and 81% and 62% for cases of OM due to M. catarrhalis and S. pyogenes, respectively.
Pneumonia: In a multicenter observational study in France comparing the periods before and after the switch from pneumococcal 7-valent conjugate vaccine to Prevenar 13, there was 16% reduction in all community acquired pneumonia (CAP) cases in emergency departments in children 1 month to 15 years of age. Reductions were 53% (p<0.001) for CAP cases with pleural effusion and 63% (p<0.001) for microbiologically confirmed pneumococcal CAP cases. In the second year after the introduction of Prevenar 13 the total number of CAP cases due to the 6 additional vaccine serotypes in Prevenar 13 was reduced by 74% (27 to 7 isolates).
In an ongoing surveillance system (2002 to 2013) to document the impact of pneumococcal 7-valent conjugate vaccine and subsequently Prevenar 13 on CAP in children less than 5 years in Southern Israel using a 2 dose primary series with a booster dose in the second year of life, there was a reduction of 68% (95% CI 73; 61) in outpatient visits and 32% (95% CI 39; 22) in hospitalizations for alveolar CAP following the introduction of Prevenar 13 when compared to the period before the introduction of pneumococcal 7-valent conjugate vaccine was introduced.
Reduction of Antimicrobial Resistance (AMR): Following the introduction of pneumococcal 7-valent conjugate vaccine and subsequently Prevenar 13, a reduction in AMR has been shown as a result of direct reduction of serotypes and clones associated with AMR from the population (including 19A), reduction of transmission (herd effects), and reduction in the use of antimicrobial agents.
In a double-blind, randomized, controlled study in Israel comparing pneumococcal 7-valent conjugate vaccine and Prevenar 13 that reported the acquisition of S. pneumoniae, reductions of serotypes 19A, 19F, and 6A not susceptible to either penicillin, erythromycin, clindamycin, penicillin plus erythromycin, or multiple drugs (≥3 antibiotics) ranged between 34% and 62% depending on serotype and antibiotic.
Analyses of data from the United States Centers for Disease Control and Prevention evaluated temporal trends for four antibiotic classes and showed that compared to 2009 (the last year of pneumococcal 7-valent conjugate vaccine use in the US, following which it was replaced with Prevenar 13), by 2013 the annual incidence of IPD due to pneumococci non-susceptible to macrolides, cephalosporins, penicillins, and tetracyclines had decreased by 63%, 81%, 83%, and 81% in children less than 5 years of age and 24%, 49%, 57%, and 53% in persons 65 years of age and older.
Prevenar 13 Effect on Nasopharyngeal Carriage: In a surveillance study in France in children presenting with acute otitis media, changes in nasopharyngeal (NP) carriage of pneumococcal serotypes were evaluated following the introduction of pneumococcal 7-valent conjugate vaccine and subsequently Prevenar 13. Prevenar 13 significantly reduced NP carriage of the 6 additional serotypes (and serotype 6C) combined and individual serotypes 6C, 7F, 19A when compared with pneumococcal 7-valent conjugate vaccine. A reduction in carriage was also seen for serotype 3 (2.5% vs. 1.1%; p=0.1). There was no carriage of serotypes 1 and 5 observed.
The effect of pneumococcal conjugate vaccination on nasopharyngeal carriage was studied in a randomised double-blind study in which infants received either Prevenar 13 or pneumococcal 7-valent conjugate vaccine at 2, 4, 6 and 12 months of age in Israel. Prevenar 13 significantly reduced newly identified NP acquisition of the 6 additional serotypes (and serotype 6C) combined and of individual serotypes 1, 6A, 6C, 7F, 19A when compared with pneumococcal 7-valent conjugate vaccine. There was no reduction seen in serotype 3 and for serotype 5 the colonization was too infrequent to assess impact. For 6 of the remaining 7 common serotypes, similar rates of NP acquisition were observed in both vaccine groups; for serotype 19F a significant reduction was observed.
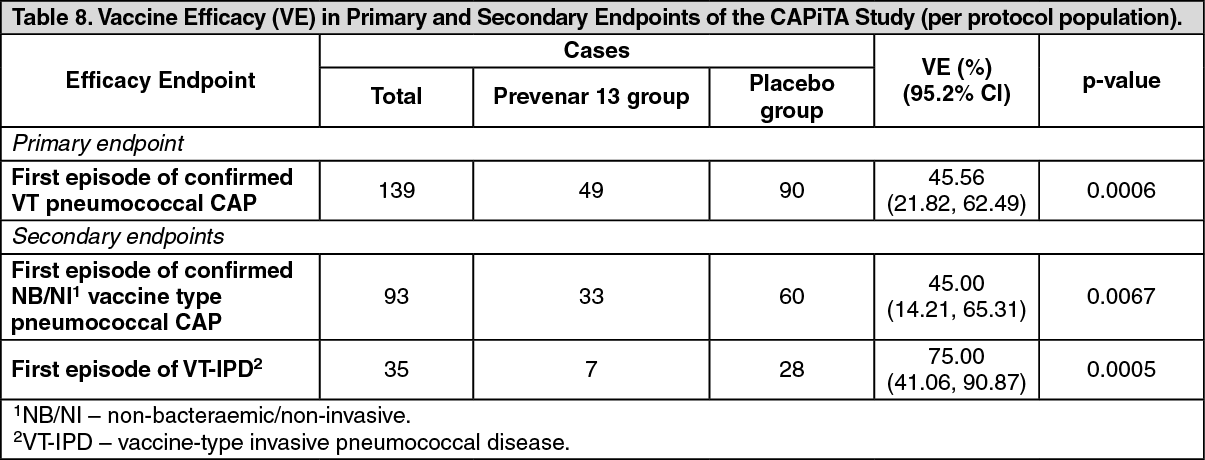
Efficacy Study in Adults 65 Years and Older: Efficacy against vaccine type (VT) pneumococcal CAP and IPD was assessed in a large-scale randomized double-blind, placebo controlled study (Community-Acquired Pneumonia Immunization Trial in Adults-CAPiTA) in the Netherlands. 84,496 subjects, 65 years and older received a single vaccination of either Prevenar 13 or placebo in a 1:1 randomization.
Efficacy of Prevenar 13 in preventing a first episode of VT pneumococcal CAP (the primary endpoint of the study) and the two secondary endpoints was demonstrated as shown in Table 5. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe protective efficacy of Prevenar 13 against a first episode of VT pneumococcal CAP, VT NB/NI pneumococcal CAP, and VT-IPD was evident shortly after vaccination and was sustained throughout the duration of the study.
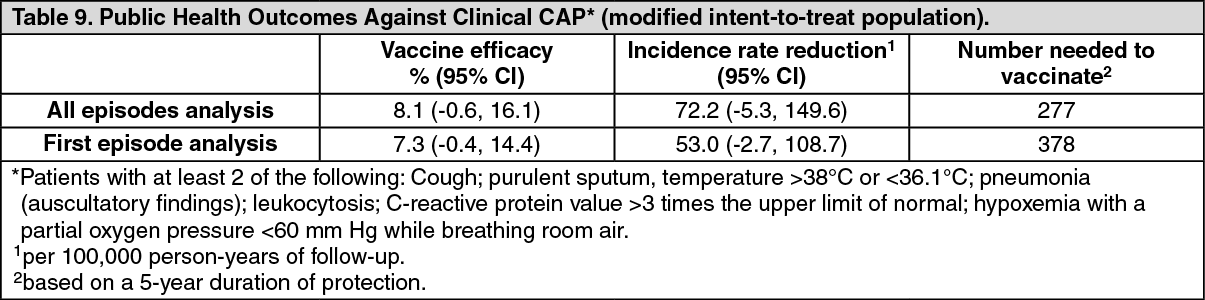
A post-hoc analysis was used to estimate the following public health outcomes against clinical CAP (as defined in the CAPiTA study, and based on clinical findings regardless of radiologic infiltrate or etiologic confirmation): vaccine efficacy, incidence rate reduction and number needed to vaccinate (see Table 9).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAlthough CAPiTA was not powered to demonstrate serotype specific VE, an evaluation of clinical CAP data was performed for serotypes with at least 10 outcomes in the placebo group. VE (95% CI) for the five evaluated serotypes against first clinical CAP episodes were: serotype 1, 20.0% (-83.1% to 65.8%); serotype 3, 61.5% (17.6% to 83.4%); serotype 6A, 33.3% (-58.6% to 73.2%); serotype 7F, 73.3% (40.5% to 89.4%); and serotype 19A, 45.2% (-2.2% to 71.5%).
Immune Responses in Special Populations: Individuals with the conditions described as follows have an increased risk of pneumococcaldisease.
Sickle cell disease: An open-label, single-arm study (6096A1-3014 [B1851013]) with 2 doses of Prevenar 13 given 6 months apart was conducted in 158 children and adolescents ≥6 to <18 years of age with sickle cell disease who were previously vaccinated with 1 or more doses of PPSV23 at least 6 months prior to enrollment. After the first vaccination, Prevenar 13 elicited antibody levels measured by both IgG GMCs and OPA GMTs that were statistically significant higher when compared to levels prior to vaccination. After the second dose immune responses were comparable to the ones after the first dose. One (1) year after the second dose, antibody levels measured by both IgG GMCs and OPA GMTs were higher than levels prior to the first dose of Prevenar 13, except the IgG GMC for serotype 3 that was similar.
Additional pneumococcal 7-valent conjugate vaccine immunogenicity data: children with sickle cell disease: The immunogenicity of pneumococcal 7-valent conjugate vaccine has been investigated in an open-label, multicenter study (0887X1-100722) in 49 infants with sickle cell disease. Children were vaccinated with pneumococcal 7-valent conjugate vaccine (3 doses 1 month apart from the age of 2 months), and 46 of these children also received a PPSV23 at the age of 15-18 months. After primary immunization, 95.6% of the subjects had antibody levels of >0.35 μg/mL for all 7 serotypes found in pneumococcal 7-valent conjugate vaccine. A significant increase was seen in the concentrations of antibodies against the 7 serotypes after PPSV23, suggesting that immunological memory was well established.
HIV Infection: Children and adults not previously vaccinated with a pneumococcal vaccine: In study 6115A1-3002 (B1851021), HIV-infected children and adults (CD4 ≥200 cells/µL, viral load <50,000 copies/mL and free of active AIDS-related illness) not previously vaccinated with a pneumococcal vaccine received 3 doses of Prevenar 13. As per general recommendations, a single dose of PPSV23 was subsequently administered. Vaccines were administered at 1 month intervals. Immune responses were assessed in 259-270 evaluable subjects approximately 1 month after each dose of vaccine. After the first dose, Prevenar 13 elicited antibody levels, measured by both IgG GMCs and OPA GMTs that were statistically significantly higher when compared to levels prior to vaccination. After the second and third dose of Prevenar 13, immune responses were similar or higher than those after the first dose. The clinical benefit of the third doses remains uncertain.
Adults previously vaccinated with 23-valent pneumococcal polysaccharide vaccine: In study 6115A1-3017 (B1851028), immune responses were assessed in 329 HIV-infected adults ≥18 years of age (CD4+ T-cell count ≥200 cells/µL and viral load <50,000 copies/mL) previously vaccinated with PPSV23 administered at least 6 months prior to enrollment. Subjects received 3 doses of Prevenar 13, at enrollment, 6 months and 12 months after the first dose of Prevenar 13. After the first vaccination, Prevenar 13 elicited antibody levels measured by both IgG GMCs and OPA GMTs that were statistically significant higher when compared to levels prior to vaccination. After the second and third dose of Prevenar 13, immune responses were comparable or higher than those after the first dose. Subjects who received 2 or more previous doses of PPSV23 showed a similar immune response compared with subjects who received a single previous dose. The clinical benefit of the second and third doses remains uncertain.
Hematopoietic stem cell transplant: In study 6115A1-3003 (B1851022), children and adults with an allogeneic HSCT at ≥2 years of age received 3 doses of Prevenar 13 with an interval of at least 1 month between doses. The first dose was administered at 3 to 6 months after HSCT. A fourth (booster) dose of Prevenar 13 was administered 6 months after the third dose. As per general recommendations, a single dose of PPSV23 was administered 1 month after the fourth dose of Prevenar 13. Immune responses as measured by IgG GMCs were assessed in 168-211 evaluable subjects approximately 1 month after vaccination. Prevenar 13 elicited increased antibody levels after each dose of Prevenar 13. Immune responses after the fourth dose of Prevenar 13 were significantly increased for all serotypes compared with after the third dose.
This study demonstrated that 4 doses of Prevenar 13 elicited serum IgG concentrations similar to those induced by a single dose in healthy individuals of the same age group.
Study of Prevenar 13 containing the preservative 2-phenoxyethanol (2-PE): (note that this study applies only to Multi Dose Vials).
Safety and immunogenicity of Prevenar 13 containing the preservative 2-PE (presented in a multidose vial) given to healthy infants at 8, 12 and 16 weeks of age was compared to that of Prevenar 13 without added preservative (250 infants per group).
Pneumococcal immune responses were compared using non-inferiority criteria including the percentage of subjects with serum anti-polysaccharide serotype-specific IgG ≥0.35 μg/mL and the comparison of IgG GMCs one month after the infant series. In addition, OPA GMTs between subjects receiving Prevenar 13 with or without 2-PE were compared.
Non-inferiority for the proportion of subjects achieving an IgG concentration ≥0.35 μg/mL was demonstrated for all 13 serotypes (lower bound of the 97.5% confidence interval (CI) for the difference in percentage of responders at 0.35 μg/mL between groups was >-10%). Additionally, all 13 serotypes met the pre-defined non-inferiority criterion for IgG GMCs (lower limit of the 97.5% CI of GMR was greater than 0.5).
Correspondingly, OPA GMTs were similar in both groups, except for serotype 3, which was lower, and serotype 18C, which was higher, in the group that received Prevenar 13 with 2-PE.
Prevenar 13 Immunogenicity Clinical Trials in Adults: An antipolysaccharide binding antibody IgG level to predict protection against IPD or non-bacteremic pneumonia has not been defined for adults. However, nonclinical and clinical data support functional antibody, measured by OPA assay, as a contributor to protection against pneumococcal disease. OPA provides an in vitro measurement of the ability of serum antibodies to eliminate pneumococci by promoting complement-mediated phagocytosis and is believed to reflect relevant in vivo mechanisms of protection against pneumococcal disease. OPA titers are expressed as the reciprocal of the highest serum dilution that reduces survival of the pneumococci by at least 50%. Pivotal trials for Prevenar 13 were designed to show that functional OPA antibody responses for the Prevenar 13 serotypes are non-inferior and for some serotypes superior to the common serotypes in the currently licensed PPSV23.
Serotype-specific OPA geometric mean titers (GMTs) measured 1 month after each vaccination were calculated. Non-inferiority between vaccines was defined as the lower bound of the 2-sided, 95% confidence interval (CI) for the ratio of the GMTs (GMR) >0.5 (2-fold criterion); statistically significantly greater responses were defined as the lower bound of the 2-sided 95% CI for the GMR >1.
The response to the additional serotype 6A, which is unique to Prevenar 13 but not in PPSV23 was assessed by demonstration of a 4-fold increase in the specific OPA titer above pre-immunization levels. Superiority of the response for Prevenar 13 was defined as the lower bound of the 2-sided, 95% CI for the difference in percentages of adults achieving a 4-fold increase in OPA titer greater than zero. For comparison of OPA GMTs, a statistically greater response for serotype 6A was defined as the lower bound of the 2-sided 95% CI for the GMR >2.
Five Phase 3 clinical trials (6115A1-004, 6115A1-3005, 6115A1-3010, 6115A1-3001, 6115A1-3008) were conducted in a number of European countries and in the US evaluating the immunogenicity of Prevenar 13 in different age groups, and in individuals who were either not previously vaccinated (PPSV23 unvaccinated) with PPSV23 or had received 1 or more doses of PPSV23 (PPSV23 pre-vaccinated).
Each study included healthy adults and immunocompetent adults with stable underlying conditions including chronic cardiovascular disease, chronic pulmonary disease, renal disorders, diabetes mellitus, chronic liver disease including alcoholic liver disease, and alcoholism because it is known that these are common conditions in adults that increase risk of serious pneumococcal CAP and IPD.
Two (2) pivotal non-inferiority trials were conducted in which Prevenar 13 response was compared to PPSV23 immune response, 1 in PPSV23 unvaccinated adults aged 50-64 years (6115A1-004), and 1 in PPSV23 pre-vaccinated adults aged ≥70 years (6115A1-3005). One study (6115A1-3000) in PPSV23 pre-vaccinated adults collected safety data only. Two (2) studies (6115A1-3001 and 6115A1-3008) assessed the concomitant administration of Prevenar 13 with seasonal TIV.
Clinical trials conducted in adults not previously vaccinated with PPSV23: In an active-controlled modified double-blind clinical trial (6115A1-004) of Prevenar 13 in the US, PPSV23-unvaccinated adults aged 60 to 64 years were randomly assigned (1:1) to receive Prevenar 13 or PPSV23. In addition, adults aged 50 to 59 years were enrolled and received 1 dose of Prevenar 13 (open-label).
The OPA antibody responses elicited by Prevenar 13 were non-inferior to those elicited by PPSV23 for the 12 serotypes in common to both vaccines. In addition, 8 of the serotypes in common exhibited a statistically significantly greater immune response after Prevenar 13 compared with after PPSV23.
For serotype 6A, which is unique to Prevenar 13, the proportions of adults with a 4-fold increase after Prevenar 13 (88.5%) were significantly greater than after PPSV23 (39.2%) in PPSV23-unvaccinated adults aged 60-64 years. OPA GMTs for serotype 6A were statistically significantly greater after Prevenar 13 compared with after PPSV23.
The OPA responses elicited by Prevenar 13 in adults aged 50-59 years were non-inferior to the Prevenar 13 responses in adults aged 60-64 years for all 13 serotypes. In addition, 9 of the 13 serotypes exhibited a statistically significantly greater immune response in adults aged 50-59 years compared with adults aged 60-64 years.
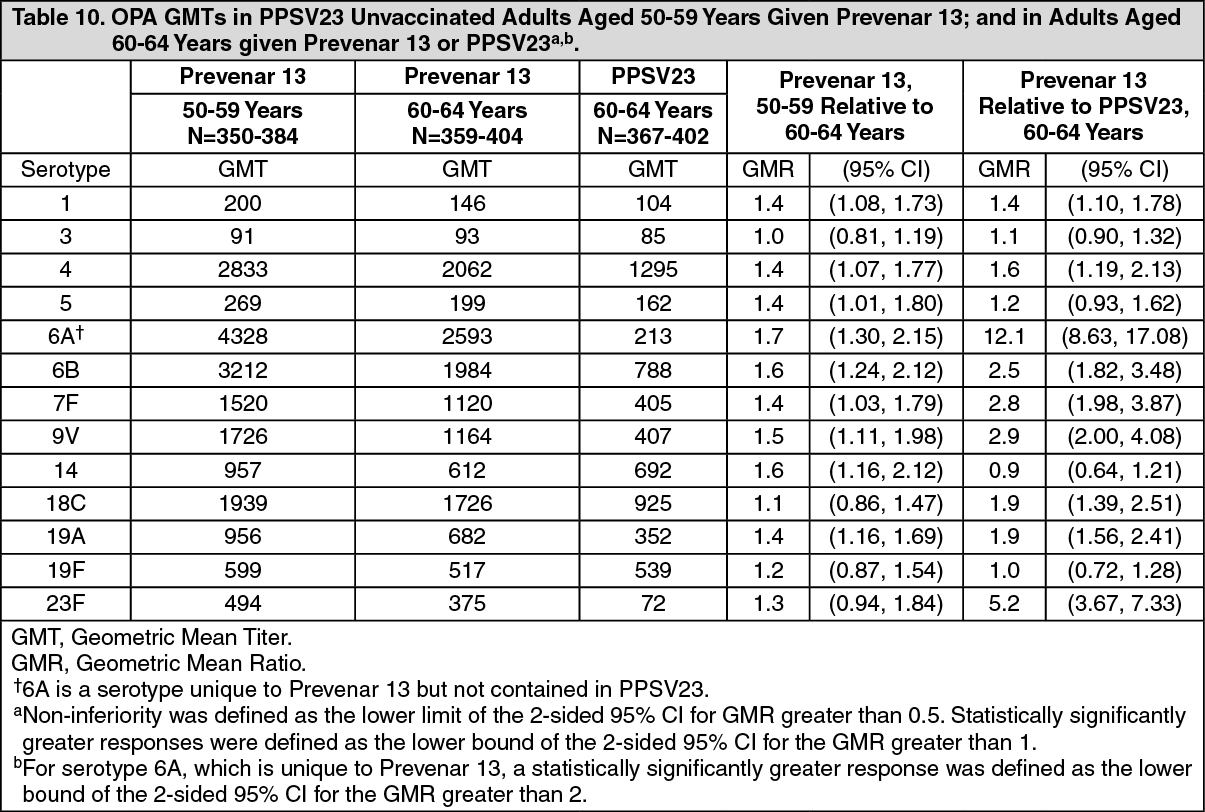
This clinical trial demonstrated that the immune responses elicited by Prevenar 13 are non-inferior and for most serotype statistically greater than PPSV23. In addition, the immune responses in adults aged 50 - 59 years were non-inferior and for most serotypes statistically significantly greater than those observed in adults aged 60 - 64 years. In adults aged 60-64 years, antibody levels one year after vaccination were greater after Prevenar 13 compared to antibody levels after PPSV23 for 7 of 12 serotypes in common. In adults aged 50-59 years, antibody levels one year after vaccination with Prevenar 13 were greater for 12 of 13 serotypes compared to vaccination with Prevenar 13 in 60-64 year olds. (See Table 10.)
 Click on icon to see table/diagram/image
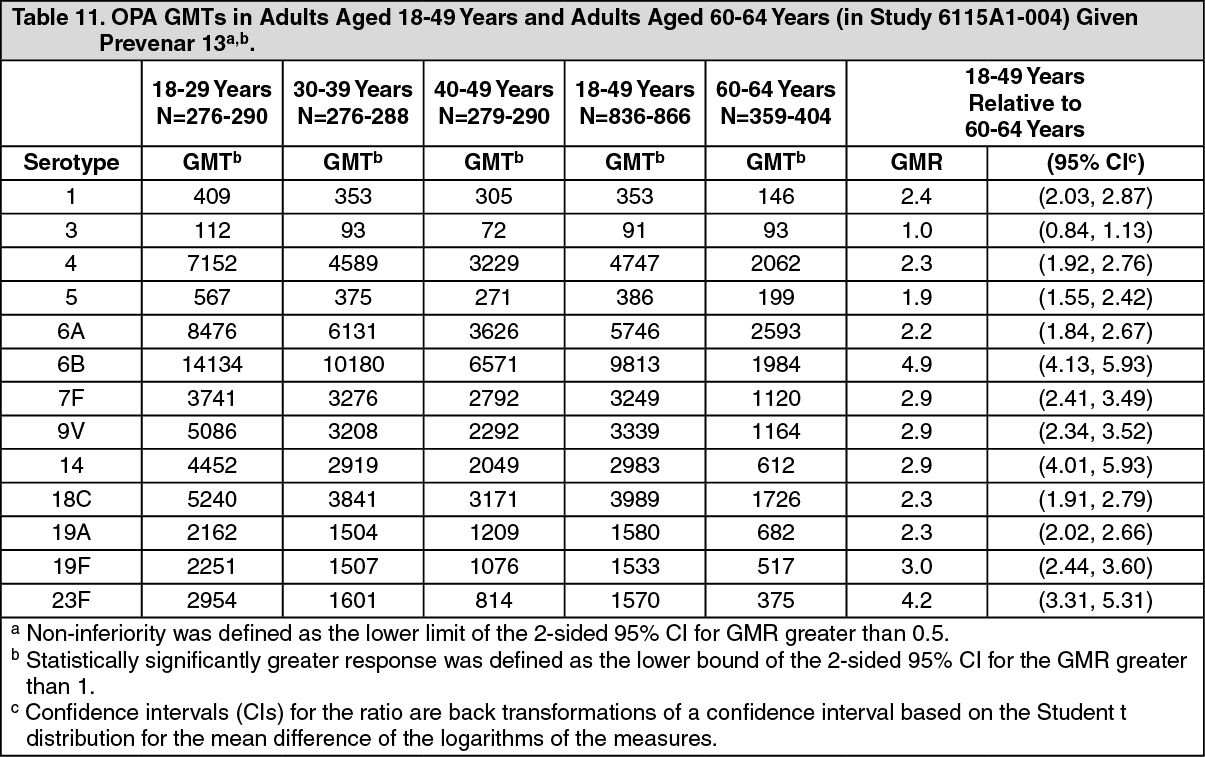
Click on icon to see table/diagram/imageTable 11 shows OPA GMTs 1 month after vaccination in subjects 18-29 years of age,30-39 years of age, and 40-49 years of age given a single dose of Prevenar 13. It also shows a comparison of OPA GMTs in subjects 18-49 years of age and 60-64 years of age. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn adults aged 18-29 years, OPA GMTs to all 13 serotypes in Prevenar 13 were non-inferior to the Prevenar 13 responses in adults aged 60-64 years. For 12 serotypes, immune responses were related to age, with adults aged 18-49 years showing statistically significantly greater responses than adults aged 60-64 years. Similarly, statistically significantly greater responses for 12 serotypes were observed for adults in age subgroups 18-29 years, 30-39 years and 40-49 years compared with adults aged 60-64 years. OPA GMTs were highest in adults aged 18-29 years and lowest in adults aged60-64 years.
One (1) year after vaccination with Prevenar 13, OPA titers had declined compared to titers measured 1 month after vaccination ranging from 23 to 2948; however, OPA titers for all serotypes remained higher than levels measured at baseline ranging from 5 to186.
Clinical trials conducted in adults previously vaccinated with PPSV23 (pre-vaccinated): In a Phase 3 active-controlled, modified double-blind clinical trial (6115A1-3005) of Prevenar 13 in the US and Sweden PPSV23-prevaccinated adults aged ≥70 years who had received 1 dose of PPSV23 ≥5 years prior were randomly assigned (1:1) to receive either Prevenar 13 or PPSV23.
The OPA antibody responses elicited by Prevenar 13 were non-inferior for the 12 serotypes in common to those elicited by PPSV23 when the vaccines were administered at a minimum of 5 years after PPSV23. In addition, 10 of the serotypes in common exhibited a statistically significantly greater immune response after Prevenar 13 compared with after PPSV23.
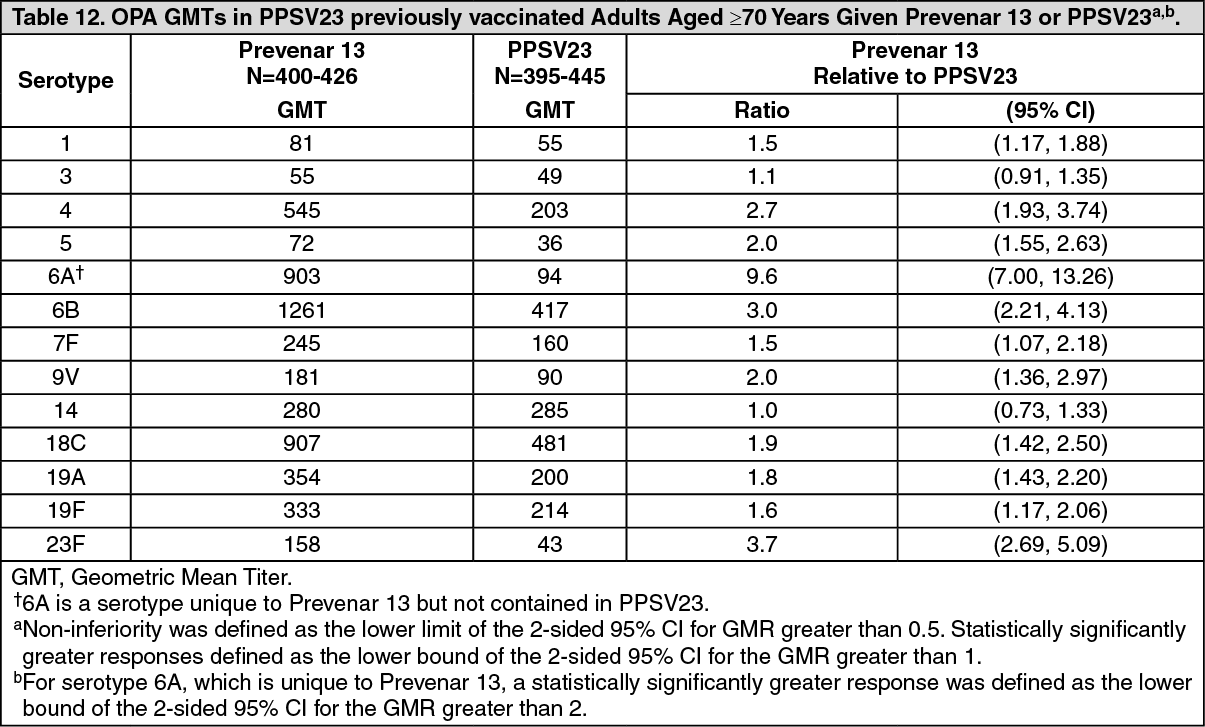
For serotype 6A, which is unique to Prevenar 13, proportions of adults with a 4-fold increase after Prevenar 13 (71.1%) was significantly greater than after PPSV23 (27.3%) in PPSV23-pre-vaccinated adults aged ≥70 years. OPA GMTs for serotype 6A were statistically significantly greater after Prevenar 13 compared with after PPSV23. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThis clinical trial demonstrated that in adults aged ≥70 years and pre-vaccinated with PPSV23 ≥5 years prior, vaccination with Prevenar 13 shows an improved immune response as compared to re-vaccination with PPSV23.
Clinical Trials to Assess Prevenar 13 Given With Seasonal TIV in Adults: Two (2) randomized, double-blind clinical trials (6115A1-3001 and 6115A1-3008) evaluated the immunogenicity of Prevenar 13 given with TIV (A/H1N1, A/H3N2, and B strains) in adults who were PPSV23 unvaccinated aged 50-59 years and in adults ≥65years.
Each clinical trial compared concomitant administration of Prevenar 13 and TIV (administered in opposite arms) with [1] TIV given with placebo and [2] with Prevenar 13 given alone. Group 1 received Prevenar 13 given with TIV, followed 1 month later by placebo; Group 2 received TIV given with placebo, followed one month later by Prevenar 13.
A Phase 3 randomized, double-blind clinical trial (6115A1-3001) of Prevenar 13 given with TIV in adults aged 50-59 years who were PPSV23 unvaccinated in the US assessed the immune responses of TIV when TIV was given with Prevenar 13 compared with TIV given with placebo (in the following called TIV alone).
A Phase 3 randomized, double-blind clinical trial (6115A1-3008) of Prevenar 13 given with TIV in adults aged ≥65 years who were PPSV23 unvaccinated in Europe assessed the immune responses of TIV when TIV was given with Prevenar 13 compared with TIV given with placebo.
Immune responses elicited by TIV were measured by haemagglutination inhibition (HAI) assays one month after TIV vaccination. The immune responses were measured as the proportion of adults achieving a ≥4-fold increase in HAI titer (responder) for each TIV strain 1 month after vaccination. The non-inferiority criterion was achieved for each vaccine antigen if the lower limit of the 95% CI for the difference in proportions of responders was >-10%.
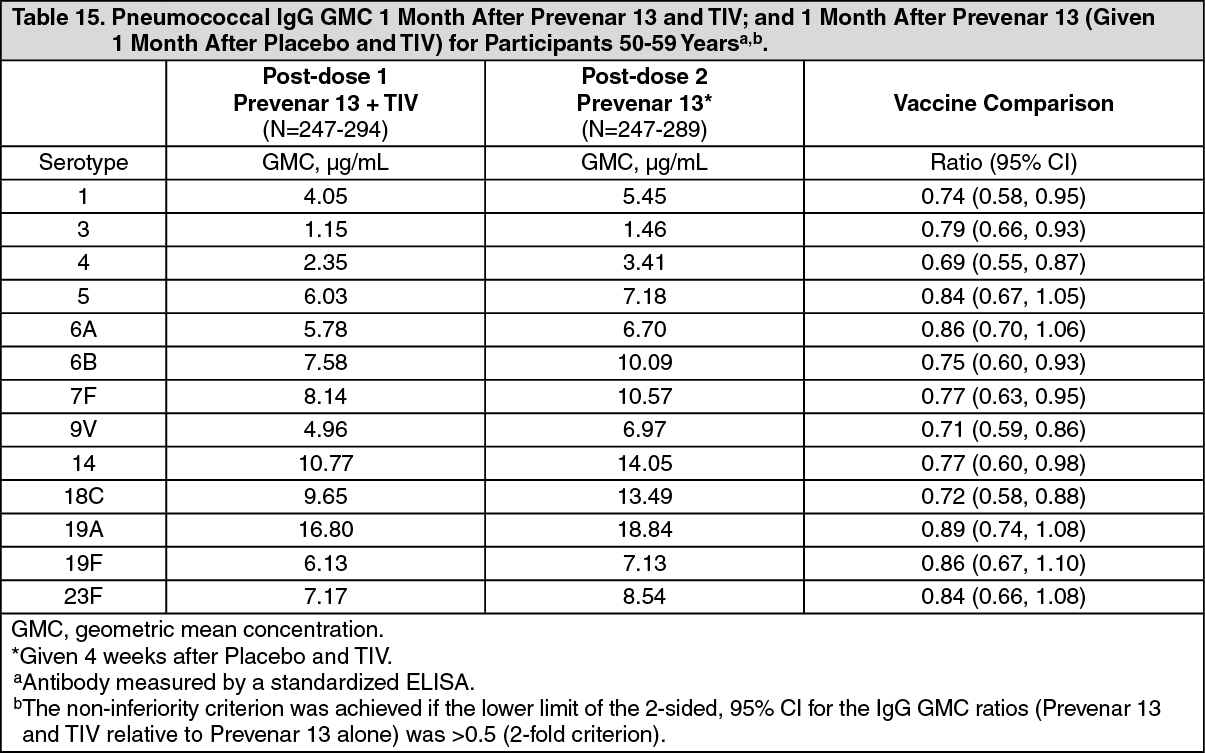
The studies also assessed the immune responses of Prevenar 13 when Prevenar 13 was given with TIV compared with Prevenar 13 given alone. The immune responses elicited by Prevenar 13 were measured by ELISA IgG GMC one month after Prevenar 13 vaccination. The non-inferiority criterion was achieved if the lower limit of the 2-sided, 95% CI for the IgG GMC ratios (Prevenar 13 and TIV relative to Prevenar 13 alone) was >0.5 (2-fold criterion).
TIV immune responses 50-59 years of age: The immune responses were similar after Prevenar 13 given concomitantly with TIV compared to TIV alone. Non-inferiority was met for all 3 TIV strains after Prevenar 13 given concomitantly with TIV compared to TIV alone (Table 13).
TIV immune responses in ≥65 years of age: Non-inferiority was met for A/H1N1, and B-strains but not for A/H3N2 with a lower limit of the 95% CI of -10.4% (Table 14). (See Table 13 and Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevenar 13 immune responses in 50-59 year olds: Non-inferiority was met for all serotypes (Table 15).
Prevenar 13 immune responses in ≥65 year olds: Non-inferiority was met for all serotypes except serotype 19F. The lower limit of the 95% CI of the GMR for 19F was 0.49 [criterion 0.5] (Table 16). (See Tables 15 and 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image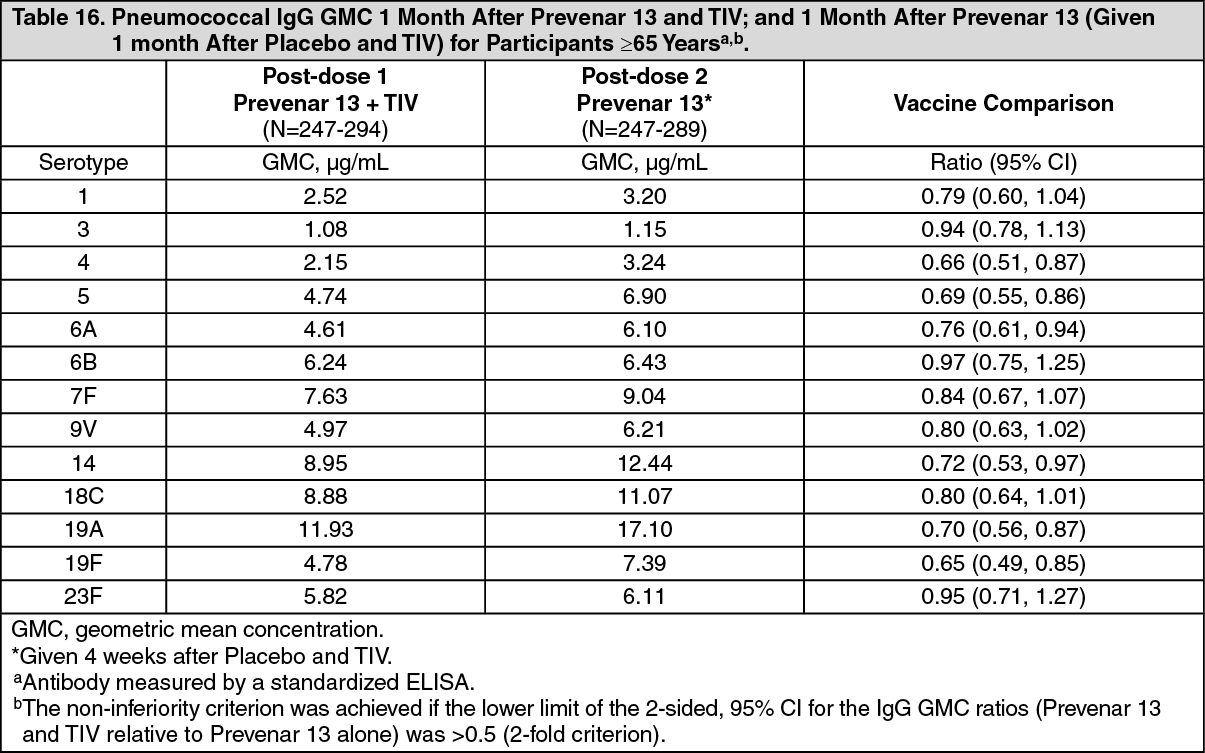 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePrevenar 13 may be given with TIV.
When Prevenar 13 was given concomitantly with TIV, the immune responses to Prevenar 13 were lower compared to when Prevenar 13 was given alone. The significance of this is unknown.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not available for vaccines.
Toxicology: Preclinical Safety Data: Studies with a vaccine formulation representative of Prevenar 13 revealed no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, juvenile toxicity and local tolerance.